 Learn more about Wellable's all-in-one
employee engagement platform
Learn more about Wellable's all-in-one
employee engagement platform




The AI Token Gold Rush Is Over (At Least for Tesla). Now What?
Wellable Weekly breaks down Tesla's new $200/week AI token cap, Starbucks' bet to replace hundreds of millions in software spend using AI, and what Gartner's prediction that one in five companies will cut half their middle managers means for the future of work.

The AI Token Gold Rush Is Over (At Least for Tesla). Now What?
Wellable Weekly breaks down Tesla's new $200/week AI token cap, Starbucks' bet to replace hundreds of millions in software spend using AI, and what Gartner's prediction that one in five companies will cut half their middle managers means for the future of work.

Best Financial Wellness Apps for Employees
Discover the best financial wellness apps for employees, from YNAB to Acorns. Plus, learn how employers can reimburse subscriptions through LSAs and wellness stipends.

Do’s & Don’ts of Modern Hiring with Kat Kibben
Wellable Weekly welcomes hiring expert and bestselling author Kat Kibben to share practical tips on writing better job postings, using AI screening tools without bias, navigating change with confidence, and what HR leaders should stop doing immediately.

Act Like an Owner: Greg Hawks on Culture, Workplace Vandals, and Leading Through Uncertainty
Wellable Weekly welcomes keynote speaker and bestselling author Greg Hawks to discuss his owner-renter-vandal framework, why engagement strategies target the wrong group, how to rebuild trust after layoffs, and what AI means for the future of work.

Remote Work Isn’t Going Away & Gen Z is “Quiet Coping”
Wellable Weekly breaks down new Stanford research showing remote work has leveled off at one in four days, why that number could shift in either direction, and what "quiet coping" in Gen Z tells employers about the mental health crisis hiding in plain sight.

How Much Does a Corporate Wellness Program Cost?
Corporate wellness program costs vary widely depending on scope. See real cost ranges, add-on fees, sample budgets, and ROI data to build your business case.

The (Not So) Hidden Bias in AI Hiring Tools
Wellable Weekly breaks down a landmark Stanford study on AI hiring bias, the "algorithmic monoculture" problem reshaping recruitment, and what Uber's decision to cut 23% of its HR team means for the future of people operations.

HR As The Culture Keeper with Jamie Jackson of HR Besties
Wellable Weekly welcomes HR Besties co-host and Chief Meme Officer Jamie Jackson to talk about why HR is villainized, how benefits are quietly eroding, navigating politics in the workplace, and what the four-day work week could mean for the future.
Remote Work: The Real Reason Gen Z Can’t Get Hired?
Wellable Weekly breaks down new Federal Reserve research linking the Gen Z unemployment surge to remote work, not AI, and what it means for early-career development, hiring decisions, and the future of in-person work.

10 Must-Ask Employee Benefits Survey Questions for Uncovering Actionable Insights
Discover 10 must-ask employee benefits survey questions that uncover what your workforce truly values—and how to turn responses into actionable improvements.

Layoffs (World Cup Edition) and the $33K Salary Gap
This Wellable Weekly episode breaks down how companies should handle layoff communication, what the US Soccer World Cup roster cut reveals about delivering bad news, and what two new surveys say about overemployment and the widening salary gap.

The Price of AI: Booed Speeches & Cut Benefits
Wellable Weekly unpacks why Gen Z graduates are booing AI commencement speakers, how companies cutting 401k matches and benefits are fueling the backlash, and what the Bolt CEO's decision to fire his entire HR team actually tells us about where the workforce is heading.

The Whoop Killer, Tokenmaxxing, and the AI Metric Trap
Wellable Weekly breaks down the Fitbit Air vs. Whoop showdown and what it means for employer wellness programs, plus what Amazon's "token maxing" scandal teaches HR leaders about AI performance metrics.

Addressing Employee Well-Being in an Era of Burnout and Uncertainty with Chase Sterling
The workforce has blown past its limits! Chase Sterling from Wellbeing Think Tank shares what's driving burnout, why AI is adding mental load, and what healthiest employers can do differently.

Workplace in Transition: The AI Investment
Are companies cutting your benefits to pay for AI? Weekly unpacks why companies are cutting parental leave, launching health fairs, and offering buyouts — and what HR leaders should do about it.

Rethinking Screenings, GLP-1s, and Smarter Health Decisions with Al Lewis
Al Lewis, a longtime critic of biometric screenings, explains why a new facial-scan technology changed his mind, plus how Quizzify's GLP-1 quiz curbs drug over-enrollment.

Digital Clones, Flat Orgs, and the Future of Hiring
Wellable Weekly breaks down Mark Zuckerberg's AI 'digital clone' project, Jack Dorsey's plan to eliminate middle management at Block, and how AI is reshaping hiring on both sides.
Gen Z, Workplace Readiness, and Economic Anxiety
Nick and Geoff unpack why Gen Z's declining social experiences are creating workplace readiness gaps, what in-person work can do about it, and how economic uncertainty is reshaping job mobility and employee sentiment.

“AI Brain Fry” Is Costing Companies More Than They Think
Wellable Weekly breaks down a new BCG study on "AI brain fry," why 1 in 5 HR employees are hitting a cognitive wall, how it differs from burnout, and what companies can do about it.

Shrinking Perks + AI Dread = Joyless Office
Wellable Weekly breaks down a WSJ report on shrinking office perks and AI dread, why companies are cutting even coffee, and how to keep AI adoption from killing team engagement.

Best Financial Wellness Apps for Employees
Discover the best financial wellness apps for employees, from YNAB to Acorns. Plus, learn how employers can reimburse subscriptions through LSAs and wellness stipends.

How Much Does a Corporate Wellness Program Cost?
Corporate wellness program costs vary widely depending on scope. See real cost ranges, add-on fees, sample budgets, and ROI data to build your business case.

10 Must-Ask Employee Benefits Survey Questions for Uncovering Actionable Insights
Discover 10 must-ask employee benefits survey questions that uncover what your workforce truly values—and how to turn responses into actionable improvements.
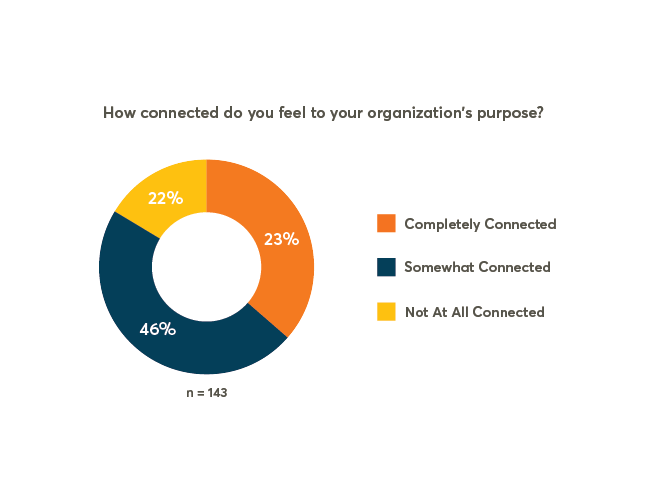
Pulse Check: 20% Of Employees Not Connected To Their Organization’s Purpose
Though employees are looking for meaningful jobs, many feel disconnected from their organization’s purpose. Explore why missions aren’t resonating with workers and learn what employers can do to better harness the power of purpose.
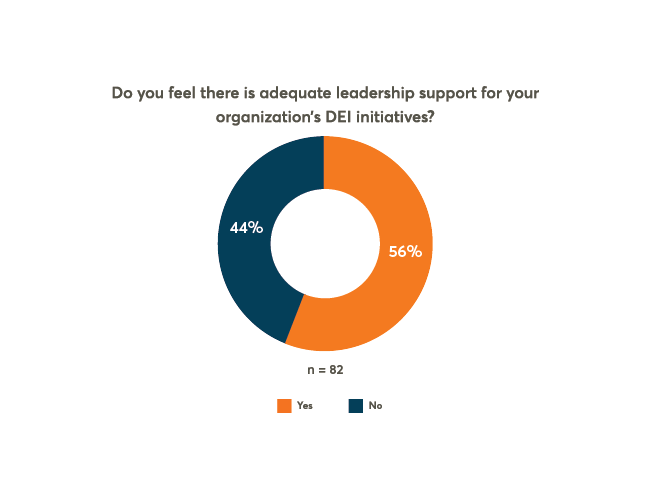
Pulse Check: 44% Of Employees Feel There Is Not Enough Leadership Support For DEIB
While most organizations have implemented DEIB strategies, employee perception of leadership support is low. Find out why and how to fix it.
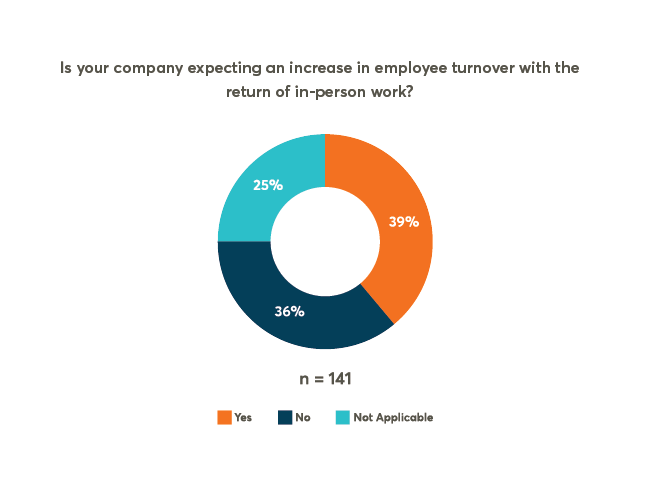
Pulse Check: Will The Return To In-Person Work Exacerbate The ‘Great Resignation’?
With resignation rates near their all-time highs, employers question whether their return-to-office plans will make matters worse. Check out these five tips for retaining talent during the transition back to in-person work.
10 Must-Ask Employee Benefits Survey Questions for Uncovering Actionable Insights
Discover 10 must-ask employee benefits survey questions that uncover what your workforce truly values—and how to turn responses into actionable improvements.
12 Best Practices for Employee Recognition Programs
Discover best practices for employee recognition programs and learn how to foster a culture of appreciation that drives engagement and performance.

20 Ways to Celebrate Work Anniversaries in 2026
Discover 20 creative ways to celebrate work anniversaries that make employees feel valued, appreciated, and motivated to stay for years to come.